Deformities
By: Courtney Hardy
An Overview
There are thousands of different types of birth defects and or deformities in children. However, there are some that are more prevalent than others. I am choosing to focus more on the structural defects or deformities, meaning areas in the body that might not have developed at all and or didn’t develop fully/functionally (Leord & Selner, 2012).
Generally speaking, women are offered an ultrasound screening at around 18 weeks of the gestational period. Most women consent to this screening. Women go through a screening process in which abnormalities such as heart defects and or others might be discovered prior to birth. There are some cases in which women can chose to have corrective surgery if applicable before the child is born, or shortly after. In other cases, if severe enough, the pregnancy might be terminated (Bergman, Carlsson, Marttala, Mattson, & Wadensten, 2015).
The three deformities I have chosen to look at are defects within the heart, cleft lip, cleft palate and clubfoot because these appear to the most common.
Heart Deformities
Types
Holes in the Heart
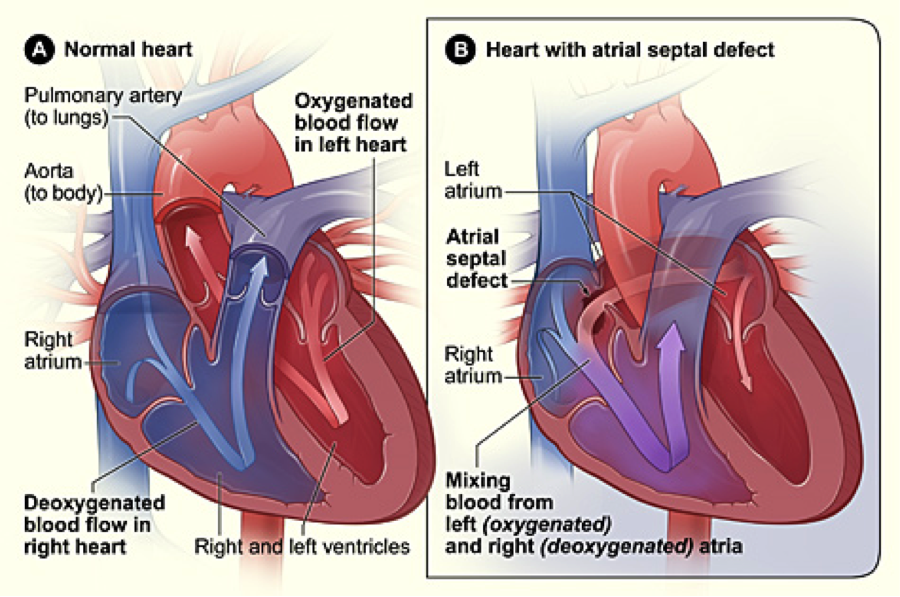
The septum is part of the hart that keeps the left and right sides of the heart apart from one another. When there are holes in the septum, the hole allows blood to mix together from both the left and the right side of the heart (“Types of Congenital Heart Defects”, 2011).
A classic form of this is Atrial septal defect otherwise known as ASD. This is when the holes in the heart allow for oxygen-rich blood flows into the right atrium (side of the heart) instead of the left one as it should (“Types of Congenital Heart Defects”, 2011).
The holes in the heart often times close on their own if not severe enough. As the child grows older, the holes find a way to close. However, if medium to large holes surgery might be necessary to treat this heart defect, using either a catheter procedure or even possibly open-heart surgery (“Types of Congenital Heart Defects”, 2011).
There are thousands of different types of birth defects and or deformities in children. However, there are some that are more prevalent than others. I am choosing to focus more on the structural defects or deformities, meaning areas in the body that might not have developed at all and or didn’t develop fully/functionally (Leord & Selner, 2012).
Generally speaking, women are offered an ultrasound screening at around 18 weeks of the gestational period. Most women consent to this screening. Women go through a screening process in which abnormalities such as heart defects and or others might be discovered prior to birth. There are some cases in which women can chose to have corrective surgery if applicable before the child is born, or shortly after. In other cases, if severe enough, the pregnancy might be terminated (Bergman, Carlsson, Marttala, Mattson, & Wadensten, 2015).
The three deformities I have chosen to look at are defects within the heart, cleft lip, cleft palate and clubfoot because these appear to the most common.
Heart Deformities
Types
Holes in the Heart
The septum is part of the hart that keeps the left and right sides of the heart apart from one another. When there are holes in the septum, the hole allows blood to mix together from both the left and the right side of the heart (“Types of Congenital Heart Defects”, 2011).
A classic form of this is Atrial septal defect otherwise known as ASD. This is when the holes in the heart allow for oxygen-rich blood flows into the right atrium (side of the heart) instead of the left one as it should (“Types of Congenital Heart Defects”, 2011).
The holes in the heart often times close on their own if not severe enough. As the child grows older, the holes find a way to close. However, if medium to large holes surgery might be necessary to treat this heart defect, using either a catheter procedure or even possibly open-heart surgery (“Types of Congenital Heart Defects”, 2011).
Patent Duct Ateriosus
This type of defect is common to most children soon after birth. Patent Ductus Arteriosus is referred to PDA. When PDA is present it means that oxygen-rich blood, which is from the aorta, combines with oxygen-poor blood from the pulmonary artery. When this happens there becomes a strain and produces pressure in the arteries of the lungs (“Types of Congenital Heart Defects”, 2011).
PDA can be treated with medicines, while others might treat themselves . However sometimes, depending on severity it can be a deformity that requires a catheter and or surgery (“Types of Congenital Heart Defects”, 2011).
Cleft Lip and Cleft Palate
What is a cleft?
When the face develops properly there are structures that form and then fuse, or bind, together. A cleft is the result of these structures not fusing. When this happens there can either be a gap in the lip or in the roof of the persons mouth (Nordqvist, 2009).
What are the types?
Cleft lip can also be known as cheiloschisis. This is a defect that effects parts of the development of the face during pregnancy. Cleft lip can be on its own, or there might also be a cleft palate, which can also be called palatoschisis, which is a similar type of defect of the face during pregnancy (Nordqvist, 2009).
The cleft lip is when the gap only affects the lip itself. There are different variations of the cleft lip. If it is a complete cleft, the gap will extend until the nose. If it is an incomplete or slight cleft might just appear as an indentation (Nordqvist, 2009).
The cleft palate however is only a gap in the palate itself. A palate consists of two parts of the skull. Of which, the hard palate are not bound together, leaving the gap. This gap may range into the jar if considered severe, while if it is considered to be incomplete the gap might simply be a hole in the roof of the mouth (Nordqvist, 2009).
This type of defect is common to most children soon after birth. Patent Ductus Arteriosus is referred to PDA. When PDA is present it means that oxygen-rich blood, which is from the aorta, combines with oxygen-poor blood from the pulmonary artery. When this happens there becomes a strain and produces pressure in the arteries of the lungs (“Types of Congenital Heart Defects”, 2011).
PDA can be treated with medicines, while others might treat themselves . However sometimes, depending on severity it can be a deformity that requires a catheter and or surgery (“Types of Congenital Heart Defects”, 2011).
Cleft Lip and Cleft Palate
What is a cleft?
When the face develops properly there are structures that form and then fuse, or bind, together. A cleft is the result of these structures not fusing. When this happens there can either be a gap in the lip or in the roof of the persons mouth (Nordqvist, 2009).
What are the types?
Cleft lip can also be known as cheiloschisis. This is a defect that effects parts of the development of the face during pregnancy. Cleft lip can be on its own, or there might also be a cleft palate, which can also be called palatoschisis, which is a similar type of defect of the face during pregnancy (Nordqvist, 2009).
The cleft lip is when the gap only affects the lip itself. There are different variations of the cleft lip. If it is a complete cleft, the gap will extend until the nose. If it is an incomplete or slight cleft might just appear as an indentation (Nordqvist, 2009).
The cleft palate however is only a gap in the palate itself. A palate consists of two parts of the skull. Of which, the hard palate are not bound together, leaving the gap. This gap may range into the jar if considered severe, while if it is considered to be incomplete the gap might simply be a hole in the roof of the mouth (Nordqvist, 2009).

Club Foot
What is it?
Club foot is described as the heels of the foot pointing downward, as the front of the foot turns inward. This also affects the muscles of the calf causing them to me smaller on the normal side, as well as causing the leg of the affected side to be slightly shorter. It would appear that generally the cause of club foot is unknown. However, in few cases club foot may appear along with other genetic syndromes such as spina bifida (Mahan, 2011).
What is it?
Club foot is described as the heels of the foot pointing downward, as the front of the foot turns inward. This also affects the muscles of the calf causing them to me smaller on the normal side, as well as causing the leg of the affected side to be slightly shorter. It would appear that generally the cause of club foot is unknown. However, in few cases club foot may appear along with other genetic syndromes such as spina bifida (Mahan, 2011).

How is it treated?
The “Ponseti” method tends to be the most common in treating club foot. This is a form of treatment that repositions the foot into how it should normally have formed. This tends to start right when the baby is born and involves a 2-3 month regimen of stretching and casting. Following that, surgery will be preformed to stretch and lengthen the tendons in the leg and foot. The last step of this method would be multiple years of having a brace on the effected foot or feet (Mahan, 2011).
The “Ponseti” method tends to be the most common in treating club foot. This is a form of treatment that repositions the foot into how it should normally have formed. This tends to start right when the baby is born and involves a 2-3 month regimen of stretching and casting. Following that, surgery will be preformed to stretch and lengthen the tendons in the leg and foot. The last step of this method would be multiple years of having a brace on the effected foot or feet (Mahan, 2011).
